Easy Methods To Care For Pes Planus
Overview
Fallen arches, or flatfoot, is a condition in which the arch on the inside of the foot is flat and the entire sole of the foot rests on the ground. It affects about 40% of the general population. Although flat feet in themselves are not usually problematic, they can create problems in the feet, hips, ankles and knees. Pain may be experienced in the lower back if there are alignment problems and if the individual is engaged in a lot of heavy, high impact activities that put stress on the bones and muscles in the lower legs. The arches of most individuals are fully developed by the age of 12 to 13. While some people are born with flat arches, for others the arches fall over time. The tibial tendon, which runs along the inside of the ankle from above the ankle to the arch, can weaken with age and with heavy activity. The posterior tendon, main support structure for the arch, can become inflamed (tendonitis) or even tear if overloaded. For women, wearing high heels can affect the Achilles tendon and alter the structure and function of the ankle. The posterior tibial tendon may compensate for this stress and break down, causing the arches to fall. Obesity is another contributing factor, as well as a serious injury to the ankle or foot, arthritis and bad circulation such as occurs with diabetes.
Causes
Fallen arches have many causes. If you have fallen arches, or flat feet, the normal arch in the middle of your foot is not curved properly. You can have this condition called ples planus in medical terms and never have any symptoms. However, fallen arches can lead to foot pain, fatigue or more serious conditions. If fallen arches alter the way you walk, you may eventually develop knee, hip and low back pain. Your foot may lose normal range of motion making it hard to rise up onto your toes. In some cases, your feet can become swollen. If you have this condition, talk to your doctor about an appropriate treatment plan.
Symptoms
A significant number of people with fallen arches (flat feet) experience no pain and have no problems. Some, however, may experience pain in their feet, especially when the connecting ligaments and muscles are strained. The leg joints may also be affected, resulting in pain. If the ankles turn inwards because of flat feet the most likely affected areas will be the feet, ankles and knees. Some people have flat feet because of a developmental fault during childhood, while others may find that the problem develops as they age, or after a pregnancy. There are some simple devices which may prevent the complications of flat feet.
Diagnosis
There are a few simple ways to assess your foot type, and most include making an imprint of your footprint. The classic way is to stand on a hard floor surface with wet feet to make a wet foot print. Look at the narrowest part of your footprint, which should be between your heel and ball of your foot. If the print of your foot in this part is less than 10% of the width of the widest part then you are likely to have high arches. more than 10% but less than 25% then your foot profile is probably normal, more than 25% or even the widest part, then you have flat feet.
Why do arches fall?
Non Surgical Treatment
Treatment often consists of giving the affected foot support from underneath so that the strain is taken off it (by the use of insoles or support pads) and so symptoms are relieved. A specialist in this problem is known as a podiatrist and these do work in the NHS - ask you father's doctor whether his condition is bad enough to warrant a referral to such a specialist.
Surgical Treatment

Surgery for flat feet is separated into three kinds: soft tissue procedures, bone cuts, and bone fusions. Depending on the severity of the flat foot, a person?s age, and whether or not the foot is stiff determines just how the foot can be fixed. In most cases a combination of procedures are performed. With flexible flat feet, surgery is geared at maintaining the motion of the foot and recreating the arch. Commonly this may involve tendon repairs along the inside of the foot to reinforce the main tendon that lifts the arch. When the bone collapse is significant, bone procedures are included to physically rebuild the arch, and realign the heel. The presence of bunions with flat feet is often contributing to the collapse and in most situations requires correction. With rigid flat feet, surgery is focused on restoring the shape of the foot through procedures that eliminate motion. In this case, motion does not exist pre-operatively, so realigning the foot is of utmost importance. The exception, are rigid flat feet due to tarsal coalition (fused segment of bone) in the back of the foot where freeing the blockage can restore function.
Prevention
Well-fitted shoes with good arch support may help prevent flat feet. Maintaining a healthy weight may also lower wear and tear on the arches.
Fallen arches, or flatfoot, is a condition in which the arch on the inside of the foot is flat and the entire sole of the foot rests on the ground. It affects about 40% of the general population. Although flat feet in themselves are not usually problematic, they can create problems in the feet, hips, ankles and knees. Pain may be experienced in the lower back if there are alignment problems and if the individual is engaged in a lot of heavy, high impact activities that put stress on the bones and muscles in the lower legs. The arches of most individuals are fully developed by the age of 12 to 13. While some people are born with flat arches, for others the arches fall over time. The tibial tendon, which runs along the inside of the ankle from above the ankle to the arch, can weaken with age and with heavy activity. The posterior tendon, main support structure for the arch, can become inflamed (tendonitis) or even tear if overloaded. For women, wearing high heels can affect the Achilles tendon and alter the structure and function of the ankle. The posterior tibial tendon may compensate for this stress and break down, causing the arches to fall. Obesity is another contributing factor, as well as a serious injury to the ankle or foot, arthritis and bad circulation such as occurs with diabetes.
Causes
Fallen arches have many causes. If you have fallen arches, or flat feet, the normal arch in the middle of your foot is not curved properly. You can have this condition called ples planus in medical terms and never have any symptoms. However, fallen arches can lead to foot pain, fatigue or more serious conditions. If fallen arches alter the way you walk, you may eventually develop knee, hip and low back pain. Your foot may lose normal range of motion making it hard to rise up onto your toes. In some cases, your feet can become swollen. If you have this condition, talk to your doctor about an appropriate treatment plan.
Symptoms
A significant number of people with fallen arches (flat feet) experience no pain and have no problems. Some, however, may experience pain in their feet, especially when the connecting ligaments and muscles are strained. The leg joints may also be affected, resulting in pain. If the ankles turn inwards because of flat feet the most likely affected areas will be the feet, ankles and knees. Some people have flat feet because of a developmental fault during childhood, while others may find that the problem develops as they age, or after a pregnancy. There are some simple devices which may prevent the complications of flat feet.
Diagnosis
There are a few simple ways to assess your foot type, and most include making an imprint of your footprint. The classic way is to stand on a hard floor surface with wet feet to make a wet foot print. Look at the narrowest part of your footprint, which should be between your heel and ball of your foot. If the print of your foot in this part is less than 10% of the width of the widest part then you are likely to have high arches. more than 10% but less than 25% then your foot profile is probably normal, more than 25% or even the widest part, then you have flat feet.
Why do arches fall?
Non Surgical Treatment
Treatment often consists of giving the affected foot support from underneath so that the strain is taken off it (by the use of insoles or support pads) and so symptoms are relieved. A specialist in this problem is known as a podiatrist and these do work in the NHS - ask you father's doctor whether his condition is bad enough to warrant a referral to such a specialist.
Surgical Treatment
Surgery for flat feet is separated into three kinds: soft tissue procedures, bone cuts, and bone fusions. Depending on the severity of the flat foot, a person?s age, and whether or not the foot is stiff determines just how the foot can be fixed. In most cases a combination of procedures are performed. With flexible flat feet, surgery is geared at maintaining the motion of the foot and recreating the arch. Commonly this may involve tendon repairs along the inside of the foot to reinforce the main tendon that lifts the arch. When the bone collapse is significant, bone procedures are included to physically rebuild the arch, and realign the heel. The presence of bunions with flat feet is often contributing to the collapse and in most situations requires correction. With rigid flat feet, surgery is focused on restoring the shape of the foot through procedures that eliminate motion. In this case, motion does not exist pre-operatively, so realigning the foot is of utmost importance. The exception, are rigid flat feet due to tarsal coalition (fused segment of bone) in the back of the foot where freeing the blockage can restore function.
Prevention
Well-fitted shoes with good arch support may help prevent flat feet. Maintaining a healthy weight may also lower wear and tear on the arches.
What Can Cause Heel Pains
Overview

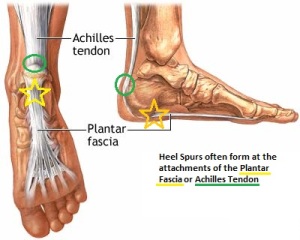
Heel pain is a very common foot problem. The sufferer usually feels pain either under the heel (planter fasciitis) or just behind it (Achilles tendinitis), where the Achilles tendon connects to the heel bone. Even though heel pain can be severe and sometimes disabling, it is rarely a health threat. Heel pain is typically mild and usually disappears on its own; however, in some cases the pain may persist and become chronic (long-term). There are 26 bones in the human foot, of which the heel (calcaneus) is the largest. The human heel is designed to provide a rigid support for the weight of the body. When we are walking or running it absorbs the impact of the foot when it hits the ground, and springs us forward into our next stride. Experts say that the stress placed on a foot when walking may be 1.25 times our body weight, and 2.75 times when running. Consequently, the heel is vulnerable to damage, and ultimately pain.
Causes
Heel pain is a common symptom that has many possible causes. Although heel pain sometimes is caused by a systemic (body-wide) illness, such as rheumatoid arthritis or gout, it usually is a local condition that affects only the foot. The most common local causes of heel pain include Plantar fasciitis. lantar fasciitis is a painful inflammation of the plantar fascia, a fibrous band of tissue on the sole of the foot that helps to support the arch. Plantar fasciitis occurs when the plantar fascia is overloaded or overstretched. This causes small tears in the fibers of the fascia, especially where the fascia meets the heel bone. Plantar fasciitis may develop in just about anyone but it is particularly common in the following groups of people: people with diabetes, obese people, pregnant women, runners, volleyball players, tennis players and people who participate in step aerobics or stair climbing. You also can trigger plantar fasciitis by pushing a large appliance or piece of furniture or by wearing worn out or poorly constructed shoes. In athletes, plantar fasciitis may follow a period of intense training, especially in runners who push themselves to run longer distances. People with flat feet have a higher risk of developing plantar fasciitis. Heel spur. heel spur is an abnormal growth of bone at the area where the plantar fascia attaches to the heel bone. It is caused by long-term strain on the plantar fascia and muscles of the foot, especially in obese people, runners or joggers. As in plantar fasciitis, shoes that are worn out, poorly fitting or poorly constructed can aggravate the problem. Heel spurs may not be the cause of heel pain even when seen on an X-ray. In fact, they may develop as a reaction to plantar fasciitis. Calcaneal apophysitis, n this condition, the center of the heel bone becomes irritated as a result of a new shoe or increased athletic activity. This pain occurs in the back of the heel, not the bottom. Calcaneal apophysitis is a fairly common cause of heel pain in active, growing children between the ages of 8 and 14. Although almost any boy or girl can be affected, children who participate in sports that require a lot of jumping have the highest risk of developing this condition. Bursitis. ursitis means inflammation of a bursa, a sac that lines many joints and allows tendons and muscles to move easily when the joint is moving. In the heel, bursitis may cause pain at the underside or back of the heel. In some cases, heel bursitis is related to structural problems of the foot that cause an abnormal gait (way of walking). In other cases, wearing shoes with poorly cushioned heels can trigger bursitis. Pump bump. his condition, medically known as posterior calcaneal exostosis, is an abnormal bony growth at the back of the heel. It is especially common in young women, in whom it is often related to long-term bursitis caused by pressure from pump shoes. Local bruises. ike other parts of the foot, the heel can be bumped and bruised accidentally. Typically, this happens as a "stone bruise," an impact injury caused by stepping on a sharp object while walking barefoot. Achilles tendonitis. n most cases, Achilles tendonitis (inflammation of the Achilles tendon) is triggered by overuse, especially by excessive jumping during sports. However, it also can be related to poorly fitting shoes if the upper back portion of a shoe digs into the Achilles tendon at the back of the heel. Less often, it is caused by an inflammatory illness, such as ankylosing spondylitis (also called axial spondylarthritis), reactive arthritis, gout or rheumatoid arthritis. Trapped nerve. ompression of a small nerve (a branch of the lateral plantar nerve) can cause pain, numbness or tingling in the heel area. In many cases, this nerve compression is related to a sprain, fracture or varicose (swollen) vein near the heel.
Symptoms
Pain in the heel can be caused by many things. The commonest cause is plantar fascitis. Other causes include, being overweight, constantly being on your feet, especially on a hard surface like concrete and wearing hard-soled footwear, thinning or weakness of the fat pads of the heel, injury to the bones or padding of the heel, arthritis in the ankle or heel (subtalar) joint, irritation of the nerves on the inner or outer sides of the heel, fracture of the heel bone (calcaneum).
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
If you have experienced painful heels try wearing your shoes around your house in the evening. Don't wear slippers or socks or go barefoot. You may also try gentle calf stretches for 20 to 30 seconds on each leg. This is best done barefoot, leaning forward towards a wall with one foot forward and one foot back. If the pain persists longer than one month, you should visit a podiatrist for evaluation and treatment. Your feet should not hurt, and professional podiatric care may be required to help relieve your discomfort. If you have not exercised in a long time, consult your podiatric physician before starting a new exercise program. Begin an exercise program slowly. Don't go too far or too fast. Purchase and maintain good shoes and replace them regularly. Stretch each foot and achilles tendon before and after exercise. Avoid uneven walking surfaces or stepping on rocks as much as possible. Avoid going barefoot on hard surfaces. Vary the incline on a treadmill during exercise. Nobody walks uphill all the time. If it hurts, stop. Don't try to "work through the pain." Your podiatric physician/surgeon has been trained specifically and extensively in the diagnosis and treatment of all manner of foot conditions. This training encompasses all of the intricately related systems and structures of the foot and lower leg including neurological, circulatory, skin, and the musculoskeletal system, which includes bones, joints, ligaments, tendons, muscles, and nerves.
Surgical Treatment
Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
heel pain in the morning
Prevention

A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don't underestimate your body's need for rest and good nutrition. If obese, lose weight.
Heel pain is a very common foot problem. The sufferer usually feels pain either under the heel (planter fasciitis) or just behind it (Achilles tendinitis), where the Achilles tendon connects to the heel bone. Even though heel pain can be severe and sometimes disabling, it is rarely a health threat. Heel pain is typically mild and usually disappears on its own; however, in some cases the pain may persist and become chronic (long-term). There are 26 bones in the human foot, of which the heel (calcaneus) is the largest. The human heel is designed to provide a rigid support for the weight of the body. When we are walking or running it absorbs the impact of the foot when it hits the ground, and springs us forward into our next stride. Experts say that the stress placed on a foot when walking may be 1.25 times our body weight, and 2.75 times when running. Consequently, the heel is vulnerable to damage, and ultimately pain.
Causes
Heel pain is a common symptom that has many possible causes. Although heel pain sometimes is caused by a systemic (body-wide) illness, such as rheumatoid arthritis or gout, it usually is a local condition that affects only the foot. The most common local causes of heel pain include Plantar fasciitis. lantar fasciitis is a painful inflammation of the plantar fascia, a fibrous band of tissue on the sole of the foot that helps to support the arch. Plantar fasciitis occurs when the plantar fascia is overloaded or overstretched. This causes small tears in the fibers of the fascia, especially where the fascia meets the heel bone. Plantar fasciitis may develop in just about anyone but it is particularly common in the following groups of people: people with diabetes, obese people, pregnant women, runners, volleyball players, tennis players and people who participate in step aerobics or stair climbing. You also can trigger plantar fasciitis by pushing a large appliance or piece of furniture or by wearing worn out or poorly constructed shoes. In athletes, plantar fasciitis may follow a period of intense training, especially in runners who push themselves to run longer distances. People with flat feet have a higher risk of developing plantar fasciitis. Heel spur. heel spur is an abnormal growth of bone at the area where the plantar fascia attaches to the heel bone. It is caused by long-term strain on the plantar fascia and muscles of the foot, especially in obese people, runners or joggers. As in plantar fasciitis, shoes that are worn out, poorly fitting or poorly constructed can aggravate the problem. Heel spurs may not be the cause of heel pain even when seen on an X-ray. In fact, they may develop as a reaction to plantar fasciitis. Calcaneal apophysitis, n this condition, the center of the heel bone becomes irritated as a result of a new shoe or increased athletic activity. This pain occurs in the back of the heel, not the bottom. Calcaneal apophysitis is a fairly common cause of heel pain in active, growing children between the ages of 8 and 14. Although almost any boy or girl can be affected, children who participate in sports that require a lot of jumping have the highest risk of developing this condition. Bursitis. ursitis means inflammation of a bursa, a sac that lines many joints and allows tendons and muscles to move easily when the joint is moving. In the heel, bursitis may cause pain at the underside or back of the heel. In some cases, heel bursitis is related to structural problems of the foot that cause an abnormal gait (way of walking). In other cases, wearing shoes with poorly cushioned heels can trigger bursitis. Pump bump. his condition, medically known as posterior calcaneal exostosis, is an abnormal bony growth at the back of the heel. It is especially common in young women, in whom it is often related to long-term bursitis caused by pressure from pump shoes. Local bruises. ike other parts of the foot, the heel can be bumped and bruised accidentally. Typically, this happens as a "stone bruise," an impact injury caused by stepping on a sharp object while walking barefoot. Achilles tendonitis. n most cases, Achilles tendonitis (inflammation of the Achilles tendon) is triggered by overuse, especially by excessive jumping during sports. However, it also can be related to poorly fitting shoes if the upper back portion of a shoe digs into the Achilles tendon at the back of the heel. Less often, it is caused by an inflammatory illness, such as ankylosing spondylitis (also called axial spondylarthritis), reactive arthritis, gout or rheumatoid arthritis. Trapped nerve. ompression of a small nerve (a branch of the lateral plantar nerve) can cause pain, numbness or tingling in the heel area. In many cases, this nerve compression is related to a sprain, fracture or varicose (swollen) vein near the heel.
Symptoms
Pain in the heel can be caused by many things. The commonest cause is plantar fascitis. Other causes include, being overweight, constantly being on your feet, especially on a hard surface like concrete and wearing hard-soled footwear, thinning or weakness of the fat pads of the heel, injury to the bones or padding of the heel, arthritis in the ankle or heel (subtalar) joint, irritation of the nerves on the inner or outer sides of the heel, fracture of the heel bone (calcaneum).
Diagnosis
After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests.
Non Surgical Treatment
If you have experienced painful heels try wearing your shoes around your house in the evening. Don't wear slippers or socks or go barefoot. You may also try gentle calf stretches for 20 to 30 seconds on each leg. This is best done barefoot, leaning forward towards a wall with one foot forward and one foot back. If the pain persists longer than one month, you should visit a podiatrist for evaluation and treatment. Your feet should not hurt, and professional podiatric care may be required to help relieve your discomfort. If you have not exercised in a long time, consult your podiatric physician before starting a new exercise program. Begin an exercise program slowly. Don't go too far or too fast. Purchase and maintain good shoes and replace them regularly. Stretch each foot and achilles tendon before and after exercise. Avoid uneven walking surfaces or stepping on rocks as much as possible. Avoid going barefoot on hard surfaces. Vary the incline on a treadmill during exercise. Nobody walks uphill all the time. If it hurts, stop. Don't try to "work through the pain." Your podiatric physician/surgeon has been trained specifically and extensively in the diagnosis and treatment of all manner of foot conditions. This training encompasses all of the intricately related systems and structures of the foot and lower leg including neurological, circulatory, skin, and the musculoskeletal system, which includes bones, joints, ligaments, tendons, muscles, and nerves.
Surgical Treatment
Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
heel pain in the morning
Prevention
A variety of steps can be taken to avoid heel pain and accompanying afflictions. Wear shoes that fit well-front, back, and sides-and have shock-absorbent soles, rigid shanks, and supportive heel counters. Wear the proper shoes for each activity. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm up and do stretching exercises before and after running. Pace yourself when you participate in athletic activities. Don't underestimate your body's need for rest and good nutrition. If obese, lose weight.
Structural Vs. Functional Leg Length Discrepancy
Overview
Some people have an ?apparent? LLD which may make the affected leg seem longer than the other leg. There are several factors that can contribute to this feeling. Most commonly, contractures or shortening of the muscles surrounding the hip joint and pelvis make the involved leg feel longer, even when both legs are really the same length. Additionally, contractures of the muscles around the lower back from spinal disorders (i.e. arthritis, spinal stenosis), curvatures of the spine from scoliosis, and deformities of the knee or ankle joint can make one leg seem longer or shorter. In the general public, some people have an ?apparent LLD? as long as one half inch but usually don?t notice it because the LLD occurs over time. A ?true? LLD is where one leg is actually longer than the other. Patients can have unequal leg lengths of 1/4? to 1/2? and never feel it too! You can also have combinations of ?True? and ?Apparent? LLDs. During total hip replacement surgery, the surgeon may ?lengthen? the involved leg by stretching the muscles and ligaments that were contracted, as well as by restoring the joint space that had become narrowed from the arthritis. This is usually a necessary part of the surgery because it also provides stability to the new hip joint. Your surgeon takes measurements of your leg lengths on x-ray prior to surgery. Your surgeon always aims for equal leg lengths if at all possible and measures the length of your legs before and during surgery in order to achieve this goal. Occasionally, surgeons may need to lengthen the operable leg to help improve stability and prevent dislocations as well improve the muscle function around the hip.
Causes
Leg discrepancy can develop from a medical issue in any portion of the femur or tibia. One leg may lengthen, but leg shortening is much more common. Factors that can cause leg length discrepancy include inherited growth deficiencies. Infections. A bone infection can cause delayed growth in the affected limb. Injury. If your child breaks a leg, it may be shorter once it heals. This is most likely to happen if the fracture or break was complicated, an open fracture, or an injury that affected the growth plate near the end of the bone. Alternatively, a break can cause bones to grow faster after healing, making a leg longer. Tumors. Legg-Calve-Perthes disease. This is a condition that affects the ball (femoral head) of the hip joint. The femoral head may be friable and damage easily, sometimes leading to shortening of the thigh bone. Hemihypertrophy. In children with this condition, one side of the body grows more quickly than the other. Vascular malformations. These are abnormal clusters of veins and arteries that can form close to the bone and stimulate growth. Juvenile arthritis. Inflammation from arthritis can stimulate growth in the affected leg and cause discrepancy.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
The treatment of LLD depends primarily on the diagnosed cause, the age of the patient, and the severity of the discrepancy. Non-operative treatment is usually the first step in management and, in many cases, LLD is mild or is predicted to lessen in the future, based on growth rate estimates in the two legs. In such cases, no treatment may be necessary or can be delayed until a later stage of physical maturity that allows for clearer prognostic approximation. For LLD of 2cm to 2.5cm, treatment may be as simple as insertion of a heel lift or other shoe insert that evens out leg lengths, so to speak. For more severe cases, heel lifts can affect patient comfort when walking, decrease ankle stability, and greatly increase the risk of sprains. For infants with congenital shortening of the limb, a prosthetic ? often a custom-fit splint made of polypropylene ? may be successful in treating more severe LLD without surgery. In many instances, however, a surgical operation is the best treatment for LLD.

shoe lift for leg length discrepancy
Surgical Treatment
Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age.
Some people have an ?apparent? LLD which may make the affected leg seem longer than the other leg. There are several factors that can contribute to this feeling. Most commonly, contractures or shortening of the muscles surrounding the hip joint and pelvis make the involved leg feel longer, even when both legs are really the same length. Additionally, contractures of the muscles around the lower back from spinal disorders (i.e. arthritis, spinal stenosis), curvatures of the spine from scoliosis, and deformities of the knee or ankle joint can make one leg seem longer or shorter. In the general public, some people have an ?apparent LLD? as long as one half inch but usually don?t notice it because the LLD occurs over time. A ?true? LLD is where one leg is actually longer than the other. Patients can have unequal leg lengths of 1/4? to 1/2? and never feel it too! You can also have combinations of ?True? and ?Apparent? LLDs. During total hip replacement surgery, the surgeon may ?lengthen? the involved leg by stretching the muscles and ligaments that were contracted, as well as by restoring the joint space that had become narrowed from the arthritis. This is usually a necessary part of the surgery because it also provides stability to the new hip joint. Your surgeon takes measurements of your leg lengths on x-ray prior to surgery. Your surgeon always aims for equal leg lengths if at all possible and measures the length of your legs before and during surgery in order to achieve this goal. Occasionally, surgeons may need to lengthen the operable leg to help improve stability and prevent dislocations as well improve the muscle function around the hip.
Causes
Leg discrepancy can develop from a medical issue in any portion of the femur or tibia. One leg may lengthen, but leg shortening is much more common. Factors that can cause leg length discrepancy include inherited growth deficiencies. Infections. A bone infection can cause delayed growth in the affected limb. Injury. If your child breaks a leg, it may be shorter once it heals. This is most likely to happen if the fracture or break was complicated, an open fracture, or an injury that affected the growth plate near the end of the bone. Alternatively, a break can cause bones to grow faster after healing, making a leg longer. Tumors. Legg-Calve-Perthes disease. This is a condition that affects the ball (femoral head) of the hip joint. The femoral head may be friable and damage easily, sometimes leading to shortening of the thigh bone. Hemihypertrophy. In children with this condition, one side of the body grows more quickly than the other. Vascular malformations. These are abnormal clusters of veins and arteries that can form close to the bone and stimulate growth. Juvenile arthritis. Inflammation from arthritis can stimulate growth in the affected leg and cause discrepancy.
Symptoms
If your child has one leg that is longer than the other, you may notice that he or she bends one leg. Stands on the toes of the shorter leg. Limps. The shorter leg has to be pushed upward, leading to an exaggerated up and down motion during walking. Tires easily. It takes more energy to walk with a discrepancy.
Diagnosis
The doctor carefully examines the child. He or she checks to be sure the legs are actually different lengths. This is because problems with the hip (such as a loose joint) or back (scoliosis) can make the child appear to have one shorter leg, even though the legs are the same length. An X-ray of the child?s legs is taken. During the X-ray, a long ruler is put in the image so an accurate measurement of each leg bone can be taken. If an underlying cause of the discrepancy is suspected, tests are done to rule it out.
Non Surgical Treatment
The treatment of LLD depends primarily on the diagnosed cause, the age of the patient, and the severity of the discrepancy. Non-operative treatment is usually the first step in management and, in many cases, LLD is mild or is predicted to lessen in the future, based on growth rate estimates in the two legs. In such cases, no treatment may be necessary or can be delayed until a later stage of physical maturity that allows for clearer prognostic approximation. For LLD of 2cm to 2.5cm, treatment may be as simple as insertion of a heel lift or other shoe insert that evens out leg lengths, so to speak. For more severe cases, heel lifts can affect patient comfort when walking, decrease ankle stability, and greatly increase the risk of sprains. For infants with congenital shortening of the limb, a prosthetic ? often a custom-fit splint made of polypropylene ? may be successful in treating more severe LLD without surgery. In many instances, however, a surgical operation is the best treatment for LLD.
shoe lift for leg length discrepancy
Surgical Treatment
Leg shortening is employed when LLD is severe and when a patient has already reached skeletal maturity. The actual surgery is called an osteotomy , which entails the removal of a small section of bone in the tibia (shinbone) and sometimes the fibula as well, resulting in the loss of around an inch in total height. Leg lengthening is a difficult third option that has traditionally had a high complication rate. Recently, results have improved somewhat with the emergence of a technique known as callotasis , in which only the outer portion of the bone (the cortex ) is cut, (i.e. a corticotomy ). This allows the bone to be more easily lengthened by an external fixation device that is attached to either side of the cut bone with pins through the skin. The ?ex-fix,' as it is sometimes called, is gradually adjusted by an orthopaedic surgeon, and healing can occur at the same time that the leg is being distracted , or lengthened over time. Unlike epiphysiodesis, leg lengthening procedures can be performed at almost any skeletal or chronological age.
What Is Mortons Neuroma
Overview
 A neuroma develops when a nerve is compressed, injured or pinched, causing swelling and pain. A neuroma in the area between the third and fourth toes, or between the second and third toes, is known as a Morton?s neuroma. Morton?s neuroma causes sharp, burning pain and numbness in the toes and foot. You may feel like you?ve stepped on a tiny hot coal and can?t get rid of it. At the same time, you?ll have the disconcerting experience of not being able to feel your toes. Sometimes the nerve tissue becomes so thickened you can feel or see a lump.
A neuroma develops when a nerve is compressed, injured or pinched, causing swelling and pain. A neuroma in the area between the third and fourth toes, or between the second and third toes, is known as a Morton?s neuroma. Morton?s neuroma causes sharp, burning pain and numbness in the toes and foot. You may feel like you?ve stepped on a tiny hot coal and can?t get rid of it. At the same time, you?ll have the disconcerting experience of not being able to feel your toes. Sometimes the nerve tissue becomes so thickened you can feel or see a lump.
Causes
Morton's neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by wearing shoes that are too tight, wearing shoes that place the foot in an awkward position, such as high heels, a foot that is mechanically unstable, repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton's neuroma to occur on one foot at the same time. It is rare for Morton's neuroma to occur on both feet at the same time.
Symptoms
Neuroma patients occasionally complain of a ?pins and needles? sensation that spreads through their feet, or of a feeling akin to hitting their ?funny bone.? The sensation may be described as similar to an electric shock. Some patients also say that these symptoms, as well as those listed above, will come and go, depending on what they are wearing on their feet, the activity they are doing, or on other external factors.
Diagnosis
X-rays of your affected foot will not show a neuroma, as neuromas are made up of soft tissue. X-rays may be helpful, however, in helping rule in osteoarthritis or a stress fracture as the cause of your symptoms. Ultrasonography and MRI are sometimes used to help diagnose neuromas, although they are often ineffective. The clinical diagnosis by a foot care expert with experience treating this health problem is usually the most effective way to diagnose neuromas. Your podiatrist will attempt to duplicate your neuroma symptoms by pressing on the involved nerve at various points, and he or she may try to cause a clicking of your nerve that indicates nerve enlargement.
Non Surgical Treatment
If you have Morton's neuroma, shoes with a wider toe area may be recommended. You can also take painkillers to help ease the pain. Steroid injections may also be given to treat the affected nerve. If these treatments don't work, surgery may be needed. This involves removing the thickened tissue around the nerve (and sometimes the nerve itself) to release the pressure.
Surgical Treatment
Surgery for mortons neuroma consists of either a decompression, where more space is created for the nerve or a resection, where this part of the nerve is removed completely. This will result in some permanent minor numbness. Success rates for surgical procedures to treat mortons neuroma have a high success rate.
A neuroma develops when a nerve is compressed, injured or pinched, causing swelling and pain. A neuroma in the area between the third and fourth toes, or between the second and third toes, is known as a Morton?s neuroma. Morton?s neuroma causes sharp, burning pain and numbness in the toes and foot. You may feel like you?ve stepped on a tiny hot coal and can?t get rid of it. At the same time, you?ll have the disconcerting experience of not being able to feel your toes. Sometimes the nerve tissue becomes so thickened you can feel or see a lump.Causes
Morton's neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by wearing shoes that are too tight, wearing shoes that place the foot in an awkward position, such as high heels, a foot that is mechanically unstable, repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton's neuroma to occur on one foot at the same time. It is rare for Morton's neuroma to occur on both feet at the same time.
Symptoms
Neuroma patients occasionally complain of a ?pins and needles? sensation that spreads through their feet, or of a feeling akin to hitting their ?funny bone.? The sensation may be described as similar to an electric shock. Some patients also say that these symptoms, as well as those listed above, will come and go, depending on what they are wearing on their feet, the activity they are doing, or on other external factors.
Diagnosis
X-rays of your affected foot will not show a neuroma, as neuromas are made up of soft tissue. X-rays may be helpful, however, in helping rule in osteoarthritis or a stress fracture as the cause of your symptoms. Ultrasonography and MRI are sometimes used to help diagnose neuromas, although they are often ineffective. The clinical diagnosis by a foot care expert with experience treating this health problem is usually the most effective way to diagnose neuromas. Your podiatrist will attempt to duplicate your neuroma symptoms by pressing on the involved nerve at various points, and he or she may try to cause a clicking of your nerve that indicates nerve enlargement.
Non Surgical Treatment
If you have Morton's neuroma, shoes with a wider toe area may be recommended. You can also take painkillers to help ease the pain. Steroid injections may also be given to treat the affected nerve. If these treatments don't work, surgery may be needed. This involves removing the thickened tissue around the nerve (and sometimes the nerve itself) to release the pressure.
Surgical Treatment
Surgery for mortons neuroma consists of either a decompression, where more space is created for the nerve or a resection, where this part of the nerve is removed completely. This will result in some permanent minor numbness. Success rates for surgical procedures to treat mortons neuroma have a high success rate.
Why Shoe Lifts Are The Answer To Leg Length Difference
There are two unique variations of leg length discrepancies, congenital and acquired. Congenital means you are born with it. One leg is anatomically shorter compared to the other. Through developmental phases of aging, the human brain senses the gait pattern and identifies some variance. Your body typically adapts by dipping one shoulder to the "short" side. A difference of less than a quarter inch isn't very excessive, demand Shoe Lifts to compensate and usually does not have a serious effect over a lifetime.

Leg length inequality goes mainly undiagnosed on a daily basis, however this condition is easily remedied, and can eradicate a number of instances of back pain.
Therapy for leg length inequality commonly consists of Shoe Lifts . These are typically affordable, usually being below twenty dollars, in comparison to a custom orthotic of $200 or maybe more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is easily the most widespread condition impacting men and women today. Over 80 million people experience back pain at some stage in their life. It is a problem which costs companies huge amounts of money each year due to lost time and productivity. Fresh and more effective treatment solutions are always sought after in the hope of decreasing the economic impact this condition causes.

Men and women from all corners of the earth suffer from foot ache due to leg length discrepancy. In these cases Shoe Lifts can be of very beneficial. The lifts are capable of alleviating any pain and discomfort in the feet. Shoe Lifts are recommended by numerous certified orthopaedic orthopedists.
In order to support the body in a nicely balanced fashion, feet have a vital task to play. Inspite of that, it's often the most neglected zone in the human body. Many people have flat-feet which means there is unequal force exerted on the feet. This will cause other parts of the body such as knees, ankles and backs to be impacted too. Shoe Lifts make sure that appropriate posture and balance are restored.
Leg length inequality goes mainly undiagnosed on a daily basis, however this condition is easily remedied, and can eradicate a number of instances of back pain.
Therapy for leg length inequality commonly consists of Shoe Lifts . These are typically affordable, usually being below twenty dollars, in comparison to a custom orthotic of $200 or maybe more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Back ache is easily the most widespread condition impacting men and women today. Over 80 million people experience back pain at some stage in their life. It is a problem which costs companies huge amounts of money each year due to lost time and productivity. Fresh and more effective treatment solutions are always sought after in the hope of decreasing the economic impact this condition causes.
Men and women from all corners of the earth suffer from foot ache due to leg length discrepancy. In these cases Shoe Lifts can be of very beneficial. The lifts are capable of alleviating any pain and discomfort in the feet. Shoe Lifts are recommended by numerous certified orthopaedic orthopedists.
In order to support the body in a nicely balanced fashion, feet have a vital task to play. Inspite of that, it's often the most neglected zone in the human body. Many people have flat-feet which means there is unequal force exerted on the feet. This will cause other parts of the body such as knees, ankles and backs to be impacted too. Shoe Lifts make sure that appropriate posture and balance are restored.
Proven Methods To Spot Posterior Calcaneal Spur
Overview
Bone spurs usually form around joints that have arthritis, in the vertebrae of the spine, and on the heel. When they form on the heel, they may form on the back of the heel but usually form on the bottom of the heel. Of course, this is where all of the body weight comes down with each step. Spurs on the bottom of the heel are usually most painful the first few steps out of bed each morning. The pain may lessen somewhat after walking for a few minutes, but may be intense again after sitting for a half hour or so, such as after lunch. The pain usually gets worse throughout the day as you are up on your feet more. Often the pain feels like a nail being driven through the heel into the ankle and leg.
Causes
Common causes of this bone spur in the heel are repetitive trauma to the base of the heel, obesity, poor walking/running technique, poorly fitting shoes, or hereditary conditions.

Symptoms
The vast majority of people who have heel spurs feel the asscociated pain during their first steps in the morning. The pain is quite intense and felt either the bottom or front of the heel bone. Typically, the sharp pain diminishes after being up for a while but continues as a dull ache. The pain characteristically returns when first standing up after sitting for long periods.
Diagnosis
A thorough medical history and physical exam by a physician is always necessary for the proper diagnosis of heel spurs and other foot conditions. X rays of the heel area are helpful, as excess bone production will be visible.
Non Surgical Treatment
Heel spurs and plantar fascitis are usually controlled with conservative treatment. Early intervention includes stretching the calf muscles while avoiding re-injuring the plantar fascia. Decreasing or changing activities, losing excess weight, and improving the proper fitting of shoes are all important measures to decrease this common source of foot pain. Modification of footwear includes shoes with a raised heel and better arch support. Shoe orthotics recommended by a healthcare professional are often very helpful in conjunction with exercises to increase strength of the foot muscles and arch. The orthotic prevents excess pronation and lengthening of the plantar fascia and continued tearing of this structure. To aid in this reduction of inflammation, applying ice for 10-15 minutes after activities and use of anti-inflammatory medication can be helpful. Physical therapy can be beneficial with the use of heat modalities, such as ultrasound that creates a deep heat and reduces inflammation. If the pain caused by inflammation is constant, keeping the foot raised above the heart and/or compressed by wrapping with an ace bandage will help. Corticosteroid injections are also frequently used to reduce pain and inflammation. Taping can help speed the healing process by protecting the fascia from reinjury, especially during stretching and walking.
Surgical Treatment
Though conservative treatments for heel spurs work most of the time, there are some cases where we need to take your treatment to the next level. Luckily, with today?s technologies, you can still often avoid surgery. Some of the advanced technologies to treat a Heel Spur are Platelet Rich Plasma Therapy. Platelet Rich Plasma Therapy (also known as PRP) is one of several regenerative medicine techniques that University Foot and Ankle Institute has helped bring to foot and ankle care. This amazing in-office procedure allows the growth factors in the blood to be used to actually begin the healing process again long after your body has given up on healing the area. Heel Pain Shockwave Therapy. Shockwave therapy is a non-invasive procedure done in the office that allows for new blood to get to the region of fascia damage and help with healing. Results have been excellent with more than 70 percent of patients getting relief with only one treatment. Topaz for Heal Spurs and pain. Another minimally invasive technology technique is called Coblation Surgery using a Topaz probe. This minimally invasive procedure involves controlled heating of multiple tiny needles that are inserted through the skin and into the plantar fascia. This process, like PRP and Shockwave therapy, irritates the fascia enough to turn a chronic problem back into an acute problem, greatly increasing the chances of healing. Heel Spur Surgery. Endoscopic Plantar Fasciotomy is one surgical procedure that we consider to release the tight fascia. University Foot and Ankle Institute has perfected an endoscopic (camera guided) approach for fascia release to allow rapid healing and limited downtime with minimal pain.
Prevention
You can help prevent heel spur symptoms from returning by wearing the proper shoes. Customized orthotics and insoles can help relieve pressure. It is important to perform your exercises to help keep your foot stretched and relaxed.
What Causes Heel Spur

Overview
A heel spur is caused by the displacement of calcium on the bone that forms on the underside of the heel, it may be one small bony protrusion or a collection of tiny, irregularly shaped growths on the bone of the heel, which is called the calcaneum. Heel spurs are sometimes painful, described as a knife digging into the heel and other times, a heel spur goes unnoticed and is only detected by an X-ray.
Causes
Heel spurs develop in some people that have a condition called plantar fasciitis, inflammation of the plantar fascia. Heel spurs form when the plantar fascia separates from the calcaneus. An abnormal bone growth, a hook-like spur, forms from calcium deposits that grow at the site of inflammation. Heel spurs are more common in middle-aged adults and people that have had plantar fasciitis for a long time. People with flat feet or high arches are vulnerable to heel spurs. Women who wear high-heeled shoes are more susceptible, as well.

Symptoms
An individual with the lower legs turning inward, a condition called genu valgus or "knock knees," can have a tendency toward excessive pronation. This can lead to a fallen arch and problems with the plantar fascia and heel spurs. Women tend to suffer from this condition more than men. Heel spurs can also result from an abnormally high arch. Other factors leading to heel spurs include a sudden increase in daily activities, an increase in weight, or a thinner cushion on the bottom of the heel due to old age. A significant increase in training intensity or duration may cause inflammation of the plantar fascia. High-heeled shoes, improperly fitted shoes, and shoes that are too flexible in the middle of the arch or bend before the toe joints will cause problems with the plantar fascia and possibly lead to heel spurs.
Diagnosis
Because the diagnosis of heel spurs can be confused with tarsal tunnel syndrome (as described earlier), most surgeons advocate performing a tarsal tunnel release (or at least a partial tarsal tunnel release) along with the plantar fascia release. This surgery is about 80percent successful in relieving pain in the small group of patients who do not improve with conservative treatments.
Non Surgical Treatment
The heel pain associated with heel spurs and plantar fasciitis may not respond well to rest. If you walk after a night's sleep, the pain may feel worse as the plantar fascia suddenly elongates, which stretches and pulls on the heel. The pain often decreases the more you walk. But you may feel a recurrence of pain after either prolonged rest or extensive walking. If you have heel pain that persists for more than one month, consult a health care provider. He or she may recommend conservative treatments such as stretching exercises, shoe recommendations, taping or strapping to rest stressed muscles and tendons, shoe inserts or orthotic devices, physical therapy. Heel pain may respond to treatment with over-the-counter medications such as acetaminophen (Tylenol), ibuprofen (Advil), or naproxen (Aleve). In many cases, a functional orthotic device can correct the causes of heel and arch pain such as biomechanical imbalances. In some cases, injection with a corticosteroid may be done to relieve inflammation in the area.
Surgical Treatment
More than 90 percent of people get better with nonsurgical treatments. If conservative treatment fails to treat symptoms of heel spurs after a period of 9 to 12 months, surgery may be necessary to relieve pain and restore mobility. Surgical techniques include release of the plantar fascia, removal of a spur. Pre-surgical tests or exams are required to identify optimal candidates, and it's important to observe post-surgical recommendations concerning rest, ice, compression, elevation of the foot, and when to place weight on the operated foot. In some cases, it may be necessary for patients to use bandages, splints, casts, surgical shoes, crutches, or canes after surgery. Possible complications of heel surgery include nerve pain, recurrent heel pain, permanent numbness of the area, infection, and scarring. In addition, with plantar fascia release, there is risk of instability, foot cramps, stress fracture, and tendinitis.
Prevention
The best way to prevent heel spurs is by wearing properly fitted footwear. Shoes should have a shock absorbing tread and soles and should be effective in supporting the heel and arch. Proper warm up and stretching before embarking on any physical activity that will put pressure or impact on the area is highly recommended. Also, just as it?s important for your general health, if you can lose some extra pounds, you will be more likely to avoid heel spurs. If you are starting to feel the onset of pain, it may not be heel spurs, but could be a tendonitis condition that could lead to heel spurs.