What Is Heel Discomfort

Overview
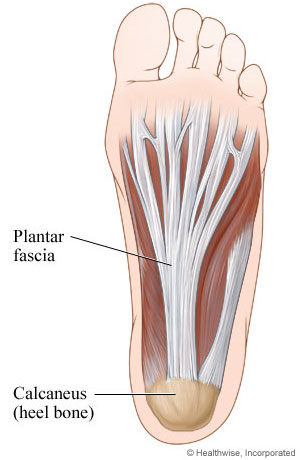
Plantar fasciitis was previously believed to be inflammation of the fascia near its insertion on the heel bone. The suffix (-itis) means inflammation. Studies, however, reveal that changes in the tissue associated with the injury are degenerative and not related to inflammation, at least not in the way most people typically think of inflammation. Sudden onset of heel pain may indeed be related to acute inflammation. For persistent heel pain the condition more closely resembles long-standing degeneration of the plantar fascia near its attachment than inflammation. This could explain why anti-inflammatory medications and injections have been unsuccessful at treating it. But there is more to heel pain than just the plantar fascia.
Causes
Plantar fasciitis tends to strike those who overtrain, neglect to stretch their calf muscles, or overdo hill work and speedwork. Plantar fasciitis can also be caused by biomechanical flaws, including flat, high-arched feet and a tight Achilles tendon; excessive pronation; sudden increases in training mileage; beginning speedwork; wearing worn running shoes; running on hard surfaces, like asphalt or concrete; or wearing high heels all day before switching into flat running shoes.
Symptoms
Heel pain is the most common symptom associated with plantar fasciosis. Your heel pain may be worse in the morning or after you have been sitting or standing for long periods. Pain is most common under your heel bone, but you also may experience pain in your foot arch or on the outside aspect of your foot. Other common signs and symptoms of plantar fasciosis include mild swelling and redness in your affected area, tenderness on the bottom of your heel, impaired ability to ambulate.
Diagnosis
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose plantar fasciitis. Occasionally, further investigations such as an X-ray, ultrasound or MRI may be required to assist with diagnosis and assess the severity of the condition.
Non Surgical Treatment
Teatment of plantar fasciitis can be a long and frustrating process for both the coach and athlete. If you do not have a firm grasp of the goals of this rehabilitation program your best advice will be to find a professional who routinely deals with athletic injuries. The "down time" for plantar fasciitis will be at least six weeks and up to six months of conservative care before drastic measures like surgery should be considered. The goal of this rehab program is to initially increase the passive flexion of the foot eventually leading to improvements in dynamic balance and flexibility of the foot and ankle, followed by a full return to function.
Surgical Treatment
When more-conservative measures aren't working, your doctor might recommend steroid shots. Injecting a type of steroid medication into the tender area can provide temporary pain relief. Multiple injections aren't recommended because they can weaken your plantar fascia and possibly cause it to rupture, as well as shrink the fat pad covering your heel bone. Extracorporeal shock wave therapy. In this procedure, sound waves are directed at the area of heel pain to stimulate healing. It's usually used for chronic plantar fasciitis that hasn't responded to more-conservative treatments. This procedure may cause bruises, swelling, pain, numbness or tingling and has not been shown to be consistently effective. Surgery. Few people need surgery to detach the plantar fascia from the heel bone. It's generally an option only when the pain is severe and all else fails. Side effects include a weakening of the arch in your foot.
Stretching Exercises
The following exercises are commonly prescribed to patients with this condition. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 2 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate and advanced exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head until you feel a stretch in the back of your calf, Achilles tendon, plantar fascia or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Resistance Band Calf Strengthening. Begin this exercise with a resistance band around your foot as demonstrated and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free.